Menstrual Cycles: Normal Variability and Clinical Terms - Physiology Flashcards
Menstrual Cycles: Normal Variability and Clinical Terms Here we'll learn about variation in the menstrual cycle, ovulation, and the fertile window, and we'll learn clinical terms used to describe common menstrual phenomenon. The physiological details
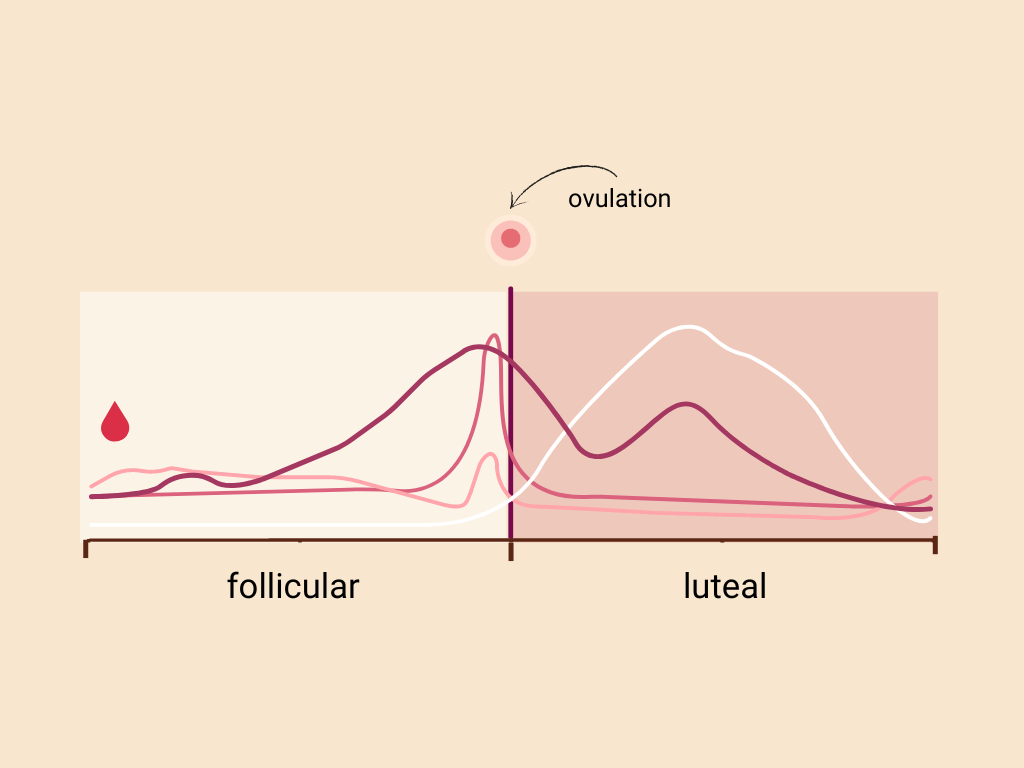
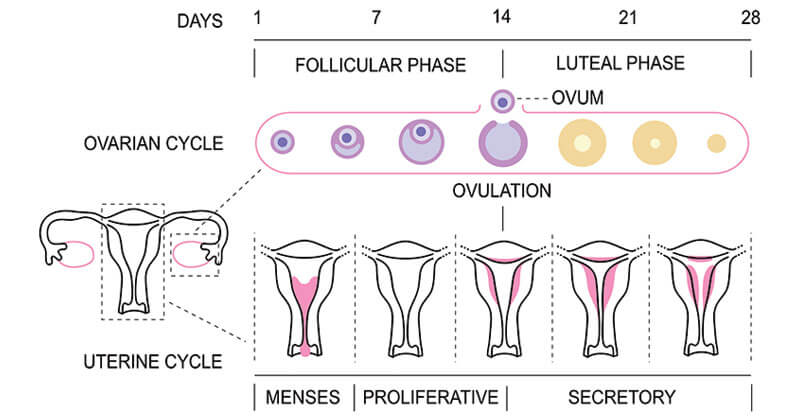
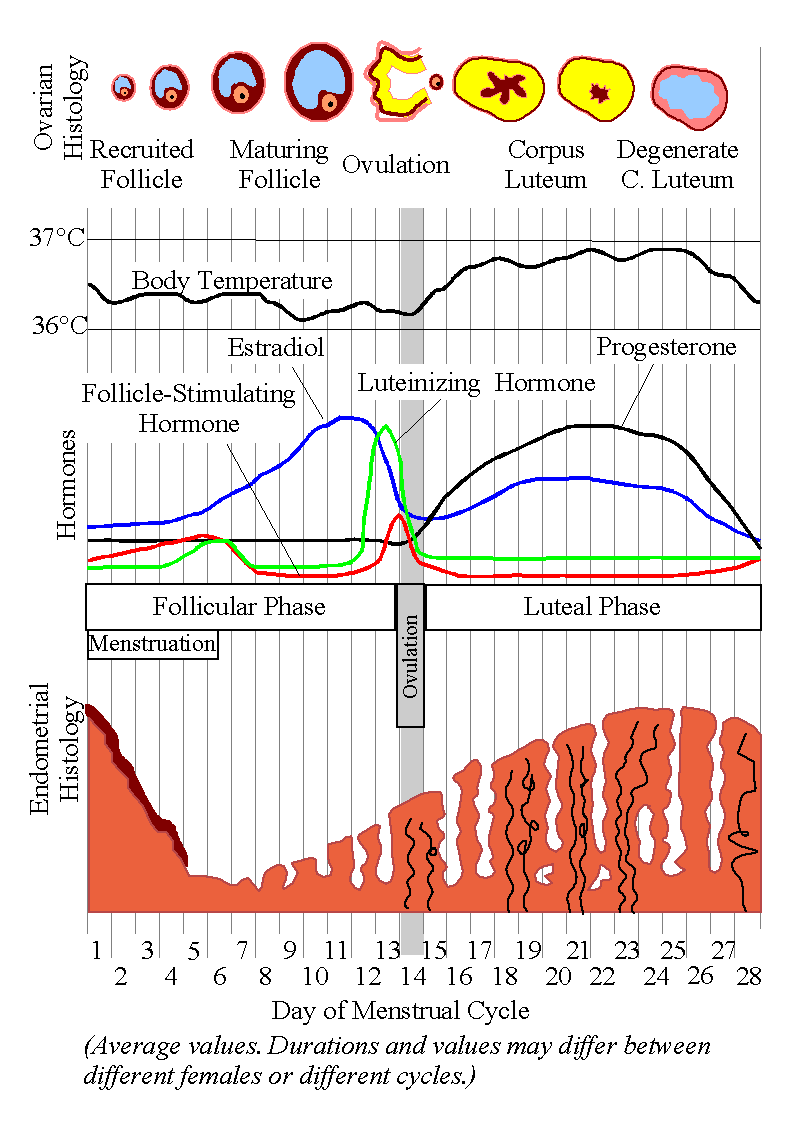
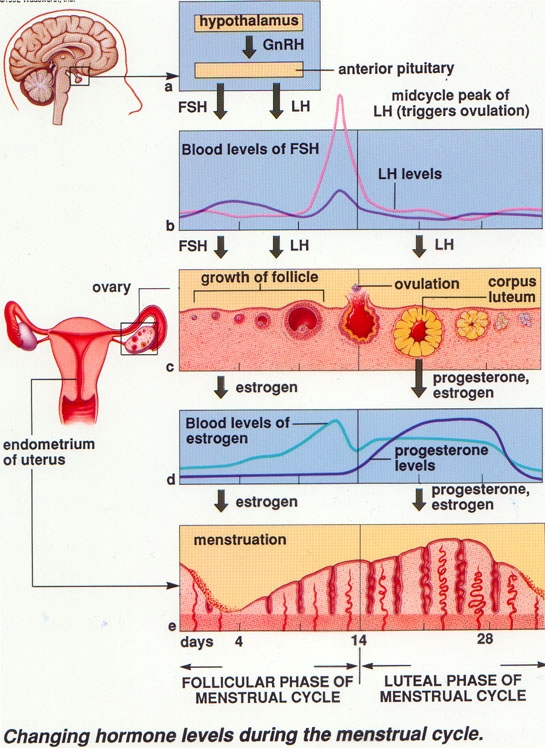
Menstrual Cycles: Normal Variability and Clinical Terms Here we'll learn about variation in the menstrual cycle, ovulation, and the fertile window, and we'll learn clinical terms used to describe common menstrual phenomenon. The physiological details regarding hormonal regulation of menstrual cycles are discussed here. A menstrual cycle begins and ends with menstruation, aka, menses (what we commonly refer to as a "period") – this is when the uterus sheds its endometrial lining. Ovarian & Uterine Cycles The ovarian cycle comprises two phases: The follicular phase, in which ovarian follicles mature and a dominant follicle emerges to prepare for ovulation. The follicular phase ends with ovulation, in which the follicle ruptures and the ova exits the ovary. After ovulation, the luteal phase begins, in which the remaining dominant follicular tissues become the corpus luteum. The Uterine Cycle comprises three phases that align with the ovarian cycle as follows: During the follicular phase of the ovarian cycle, the uterus passes through menses, when the uterine lining sheds, then through the proliferative phase, during which the endometrium begins to replace itself and grows thicker. During the luteal phase of the ovarian cycle, the corpus luteum secretes progesterone, which stimulates the endometrium and thus begins the secretory phase of the uterine cycle. During this phase, the endometrium becomes rich in glandular tissue and reaches maximal thickness, in preparation for implantation of a potential embryo. In most cases, no embryo is implanted, the corpus luteum regresses and progesterone levels fall, and the endometrial lining is again shed via menstruation. Variability in menstruation and ovulation With this basic information as a backdrop, we draw a larger diagram and add details regarding variation in menstrual cycles. Keep in mind that there is variation in the literature regarding cycle lengths, perhaps due to differences in populations and study methodology. There is significant inter-individual variation in cycle lengths: Most menstrual cycles last 23-35 days, with an average cycle length of 28 or 29 days, depending on the study. The idea that "all" or "normal" menstrual cycles are 28 days is incorrect; 28 days is simply the average that that arises from a range of cycle lengths. There is also intra-individual variation in cycle lengths: any given individual's cycle lengths vary by approximately 5 days from cycle to cycle. Variation in intra- and inter-individual cycle length is due to several factors, including age, BMI, population/ethnicity, lifestyle, and stress levels. For example, cycles within the first year or so after menarche tend to be longer, whereas the cycles during the perimenopausal years tend to be shorter. Mean bleeding duration is 4 days, +/- 1.5 days. Menstrual flow itself comprises blood, cervical mucus, vaginal secretions, and endometrial tissue. Blood lost during normal menstruation ranges from 5 to 80 mL, with an average of approximately 30 mL (note that the volume of menstrual fluid loss is higher). The follicular phase lasts approximately 17 days in an "idealized" 29-day menstrual cycle; show that a dominant ovarian follicle develops during this time. Ovulation marks the beginning of the luteal phase, which lasts approximately 12.4 days, +/- 2.4 days; during the luteal phase, the corpus luteum forms and produces progesterone. Notice that ovulation does not occur exactly midway through the cycle, nor is it always 14 days before the onset of menses, as is often assumed. The menstrual cycle begins with the first day of menses and lasts approximately 4 days, on average, followed by the proliferative phase. We show that the uterine lining is shed, along with the expelled ova, during menses, and that the uterine lining begins to regrow during the proliferative phase. Ovulation triggers the secretory phase of the uterine cycle, when the endometrium grows to its fullest thickness. If conception and implantation of an embryo has not occurred, the secretory phase ends when menses, and a new cycle, begins. Anovulation: Up to 12% of cycles in healthy, normally cycling individuals are anovulatory, meaning that an egg is not released from the ovary. Anovulation can be caused by a variety of physiological or pathological factors, including stress, pregnancy, hypothalamic-pituitary disorders, and use of combined hormonal contraceptives, which block ovulation. Learn about ovulatory dysfunction Ovulatory status is important for those who wish to either become pregnant or avoid pregnancy. However, natural variability in the lengths of the follicular and luteal phases makes it nearly impossible to predict the timing of ovulation based on dates alone. This is why the calendar method, in which sexual intercourse is avoided on certain days of the cycle, is an ineffective method of birth control. More reliable predictors of ovulation include: - Changes in basal body temperature, which falls right before ovulation and then spikes in the luteal phase. - Changes in hormones, especially luteinizing hormone, which surges and triggers ovulation. - Changes in the cervical mucus, which becomes slippery (it is often compared to an egg white). These changes may be subtle and do not always mean that ovulation occurred, but they can be helpful indicators for patients who are trying to time intercourse to increase the likelihood of pregnancy. Transvaginal ultrasound imaging is a more definitive way to see that ovulation has occurred. The fertile window, which is the approximately 6-day window when intercourse can lead to pregnancy, includes the 5 days preceding ovulation and the day of ovulation. This window is set by the lifespan of sperm cells. Sexual intercourse in the days preceding and following the fertile window are not likely to lead to pregnancy, but predicting the timing of the fertile window is difficult due to variation in the timing of ovulation. 30-50% of fertilized eggs, aka, concepti, do not implant, and are expelled in the menstrual fluid. These spontaneous abortions, or miscarriages, are most often due to genetic abnormalities that are incompatible with life, and pass without the menstruating person's awareness. We pause, here, to summarize changes in reproductive functioning during the lifespan: At one end of a line, indicate that menarche, the onset of the first menses, occurs between the ages of 10-16. At the other end of the line, indicate that menopause, the cessation of menstrual cycling, occurs between the ages of 45-55 years. At these extreme ends of the reproductive years, individuals are more likely to experience irregular cycle lengths and higher anovulatory rates. After menarche, irregularity lasts for about 12-18 months; in premenopause, irregularity increases over an average of 4 years. Be aware that although pregnancy is less likely to occur when cycles are irregular and anovulatory rates are higher, it is not impossible, and patients should be advised to use contraceptives if sexually active. Peak reproductive years last from about 18-months post-menarche to the perimenopause period. - Intra-individual cycle length varies by approximately 5 days, and up to 12% of cycles are anovulatory. - Increased irregularity in cycle length or higher anovulatory rates in these years is associated with subfertility or infertility. Clinical Terms Abnormal uterine bleeding is defined as irregularities in frequency, regularity, duration, or volume of menstrual bleeding. Heavy menstrual bleeding is defined as a blood loss of 80 mL or more, or as blood loss that negatively affects a patient's quality of life. Intermenstrual bleeding, which is another form of abnormal uterine bleeding, is uterine bleeding between defined menstrual cycles; it can occur for a variety of reasons, including hormonal changes, trauma, infection (including STIs), fibroids, polyps, or cancer. Amenorrhea is the absence of menses; it can be primary or secondary. Primary amenorrhea is the absence of menarche and menses by age 16; this is most often due to genetic abnormalities or hypothalamic-pituitary deficiencies. Secondary amenorrhea is the absence of menstruation after menarche – that is, the cessation of menstruation in someone who had been having menstrual cycles. Secondary amenorrhea is associated with pregnancy and breastfeeding, physical, nutritional or psychological stress, some contraceptives, PCOS, and ovarian failure. Dysmenorrhea is characterized by severe, sometimes debilitating, pelvic/abdominal pain during menstruation; pain may be accompanied by nausea, diarrhea, and fatigue. It can be primary or secondary. Primary dysmenorrhea is pain during menstruation caused by uterine contractions, which are induced by prostaglandins; it is thought that some patients have higher levels of prostaglandins and, thus, more pain during periods. Secondary dysmenorrhea is pain during menstruation caused by underlying disorders, such as endometriosis, fibroids, or polyps. Unfortunately, many patients suffer unnecessarily from dysmenorrhea due to the common misconception that periods are "supposed" to be extremely uncomfortable; although mild menstrual cramps are normal, severe pain that interferes with a patient's quality of life should be addressed. NSAIDs are helpful for some patients, but for others, hormonal contraceptives that limit endometrial growth, and, therefore, prostaglandin production, are a better option for pain management. For references, see full tutorial.

The phases of the menstrual cycle and associated physiological changes
Menstrual Cycle- Definition, Hormones, Phases, Diagram
Physiology of menstrual cycle

Chapter 3: The Menstrual Cycle Flashcards

theblood – Revolutionizing the Gender Data Gap
Menstrual cycle, Psychology Wiki
Physiology of menstrual cycle
Menstrual Cycle Physiology - PORTAL MyHEALTH

Pregnancy - Physiological Changes - Physiology Flashcards
Pulmonary Ventilation Rate (A-level Biology) - Study Mind

Menstrual cycle: Video, Anatomy, Definition & Function

Maternal Final Flashcards Quizlet - MATERNAL FINAL 63 studiers today 3 (9 reviews) Students also - Studocu